Cholera: Vaccines can stop the spread, but the biggest deterrent is clean water
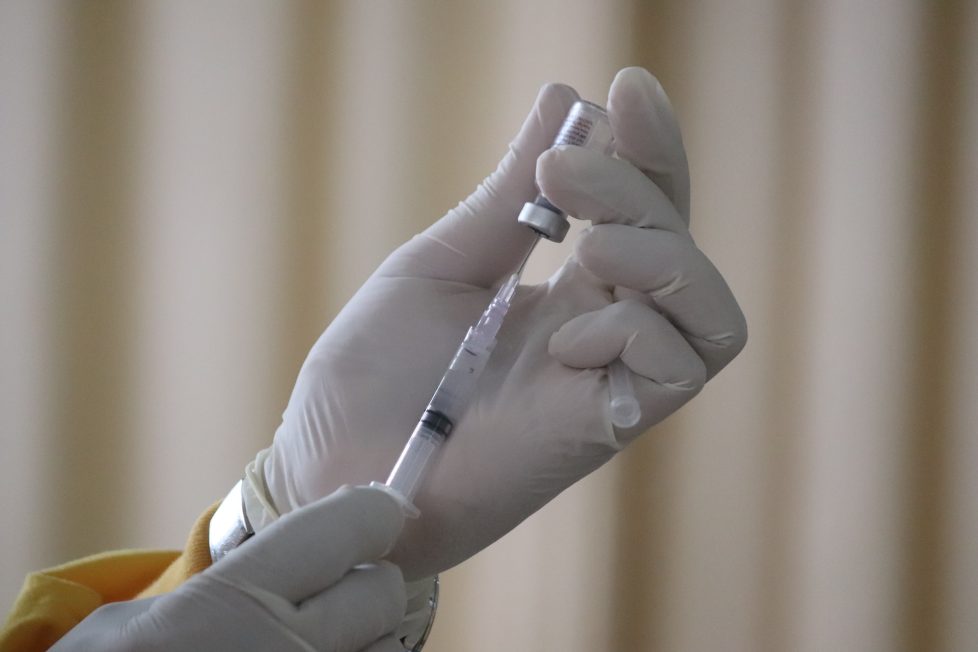
The aim of vaccination is to prevent infection with the bacterium that causes cholera: Vibrio cholerae. Vaccination can also reduce the risk of severe illness that requires hospitalisation.